McMurray’s Test
McMurray’s Test is a classic orthopedic examination to assess for meniscal tears in the knee. Specifically, the test assesses potential injury to the medial or lateral meniscus. The meniscus is a C-shaped cartilage that cushions and stabilizes the knee joint, commonly injured in twisting or traumatic movements.

How the Test is Performed
Client position: Supine (lying on their back) with the knee fully flexed.
The examiner holds the heel/foot with one hand and the knee/joint line with the other.
To test the medial meniscus:
The tibia is externally rotated (toes point outward), and a valgus stress is applied as the knee is slowly extended from a flexed position.
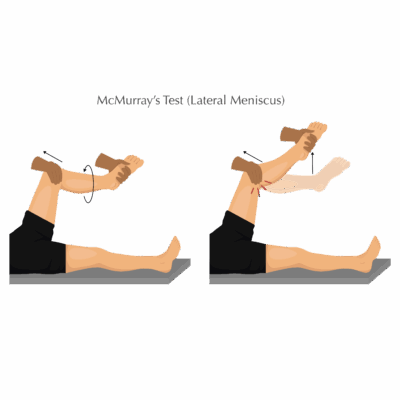
To test the lateral meniscus:
The tibia is internally rotated (toes point inward), and a varus stress is applied as the knee is extended.
-
The examiner palpates for any audible or palpable click, thud, pop, snap, or pain at the joint line during movement especially at the transition from flexion to extension.
-
A positive test: Reproduction of clicking, locking, catching, or pain (indicative of a potential meniscal tear).
Clinical Significance
-
A positive McMurray’s Test indicates possible medial or lateral meniscus tear, frequently associated with joint line pain, swelling, mechanical symptoms (locking/giving way), or history of knee trauma.
-
The test has higher specificity than sensitivity. A positive result is suggestive of a meniscal tear, but a negative test does not rule it out; MRI or further imaging may be required for confirmation.
-
Other tests, like Thessaly or Apley’s Compression, may be used alongside for comprehensive knee assessment.
Assessment
-
Use for clients with history of twisting knee injuries, mechanical symptoms, joint line pain, or persistent swelling/stiffness.
-
Document the movements which provoke symptoms/clicks and be precise about pain location and intensity for referral and treatment planning.
Treatment
-
If positive:
-
Avoid deep tissue work, direct joint mobilization, or high-force flexion/rotation at the knee, especially if mechanical symptoms or acute pain are present.
-
Focus on gentle soft tissue and pain-modifying techniques to the surrounding musculature (quads, hamstrings, calves).
-
Educate clients about avoiding deep squats, twisting, or pivoting activities until cleared by a healthcare provider.
-
Refer for further medical imaging (MRI) and evaluation by an orthopedic or physical therapist if a meniscal tear is suspected, as some tears may require surgical management.
-
Safety and Referral
-
Monitor for “red flag” signs: locked knee, severe instability, significant effusion, or pronounced movement loss, which warrant urgent referral.
-
Coordinate with the rehab team for structured progression in post-injury or post-operative cases.