Varus Stress Test (Knee)
The Varus Stress Test is an orthopedic assessment used to evaluate the integrity of the lateral collateral ligament (LCL) of the knee, as well as associated lateral structures (lateral capsular ligament, arcuate-popliteus complex). The test is performed to detect instability or injury on the outside (lateral aspect) of the knee following trauma, chronic ligament stress, or postural problems.
How the Test is Performed
-
Client position: Supine (lying on back), with the tested leg extended and relaxed.
-
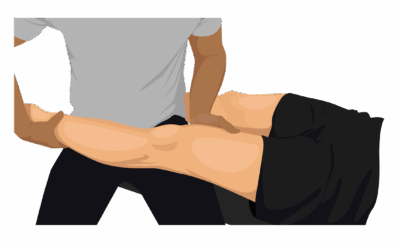
The examiner stabilizes the thigh (femur) with one hand (placed above the knee joint) and grasps the ankle or lower leg with the other.
-
The examiner applies a varus (outward) force at the ankle/lower leg while stabilizing the thigh, pushing the lower leg laterally (away from body center), to stress the lateral knee.
-
The test is performed at:
-
0° flexion (full extension): Assesses combined lateral structures (including cruciate ligaments).
-
20–30° flexion: Isolates the LCL more specifically by reducing tension on other ligaments.
-
-
Positive test: Pain on the lateral aspect of the knee and/or excessive gapping (laxity) compared to the other side.
-
Grading of instability:
-
Grade I: ≤2 mm gapping
-
Grade II: 3–5 mm (in 20° flexion only, less in extension)
-
Grade III: ≥5–10 mm (present in both flexion and extension, suggests multi-ligament injury)
-
-
Clinical Significance
-
A positive Varus Stress Test indicates LCL injury, which is less common than MCL (medial) injuries, but can occur in contact sports, trauma, or chronic postural stress.
-
Severe gapping or pain may also implicate associated structures (lateral capsule, cruciate ligaments, biceps femoris tendon, IT band), especially if present in full extension.
-
Test results help differentiate between isolated LCL injuries and more complex, multi-ligament knee injuries.
Assessment
-
Use this test for clients presenting with:
-
Lateral knee pain or instability
-
History of trauma or direct force to the inner aspect of the knee
-
Chronic lateral knee discomfort or functional instability
-
-
Document the amount of gapping, pain (and location), end-feel, and compare with the unaffected side.
Treatment
-
If positive:
-
Avoid deep tissue work, lateral mobilizations, or vigorous manual therapy to the lateral knee in acute or unstable phases.
-
Focus on gentle soft tissue techniques to reduce compensatory muscle tension in surrounding muscle groups (hamstrings, IT band, lateral calf/quad).
-
Encourage and coach rehabilitation focused on lateral knee stability, including hip abductor and lateral thigh strengthening.
-
Educate clients to avoid activities that put excessive varus (inward-to-outward) stress on the knee until stability improves.
-
Safety and Referral
-
Refer for orthopedic assessment and imaging if severe instability, multi-ligament injury, or failure to progress with conservative therapy is suspected.
-
Chronic or significant laxity may require bracing, physical therapy, or, in rare cases, surgical intervention.
-
Document progress with repeated testing and communicate findings with the care team as needed.