Upper Limb Tension Test 4 (ULTT4)
The Upper Limb Tension Test 4 (ULTT4)—also known as Elvey’s Test D or ULNT4—is a neurodynamic assessment used to evaluate the ulnar nerve and nerve roots C8–T1, which supply the medial arm, forearm, and hand.
It aims to identify nerve irritation, entrapment, or restricted neural mobility contributing to upper limb pain, numbness, or tingling. ULTT4 is often performed along with ULTT1–3 to pinpoint the nerve(s) involved.
How the Test is Performed
-
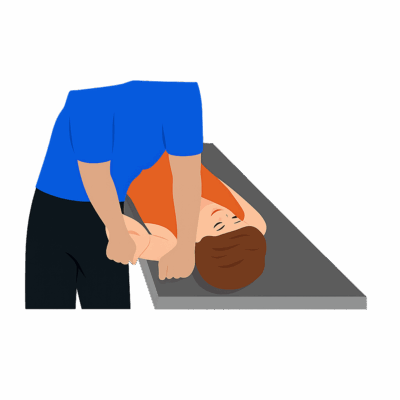
Client position: Supine, head supported, with the cervical spine in a neutral position.
-
Therapist procedure:
-
Depress the shoulder gently but firmly to tension the brachial plexus roots.
-
Abduct the shoulder to 90–110°.
-
Externally rotate the shoulder.
-
Pronate the forearm.
-
Extend the wrist, fingers, and thumb.
-
Flex the elbow, bringing the palm toward the ear (creating the characteristic “waiter’s position”).
-
Apply structural differentiation:
-
Lateral flexion of the neck away from the tested limb increases neural tension (should worsen symptoms).
-
Flexion of the neck toward the tested arm decreases tension (should ease symptoms).
-
-
-
A positive test:
-
Reproduction of tingling, numbness, or familiar pain along the ulnar nerve distribution—the medial arm, forearm, ring, and little fingers.
-
Asymmetry compared to the opposite side (range or symptom onset) also indicates dysfunction.
-
Clinical Significance
-
ULTT4 specifically assesses the ulnar nerve and its proximal segments for neural tension or entrapment at sites such as the cubital tunnel, Guyon’s canal, or cervical nerve roots C8–T1.
-
Positive results can be associated with:
-
Cubital tunnel syndrome (ulnar nerve at elbow)
-
Thoracic outlet syndrome (neural compression near clavicle or first rib)
-
Cervical radiculopathy in the lower roots (C8–T1)
-
-
Helps differentiate nerve-related arm pain from muscular, joint, or fascial tension.
Assessment
-
Use ULTT4 when clients present with:
-
Neck, elbow, or hand pain extending along the ulnar distribution (4th and 5th digits).
-
Tingling, numbness, or burning in the medial forearm or hand.
-
Weakness or poor dexterity (e.g., difficulty gripping or finger coordination).
-
-
Document:
-
Side tested, client symptoms, and shoulder/elbow position at onset.
-
Differences in movement or severity compared to the unaffected side.
-
Distribution and type of sensation reported (pins-and-needles, pain, etc.).
-
Treatment
-
If positive:
-
Avoid compressive, deep, or aggressive work along the ulnar nerve pathway (medial elbow, forearm, or hypothenar region).
-
Focus treatment on gentle fascial techniques, myofascial release, and postural correction for surrounding musculature (scalenes, pec minor, subclavius, and forearm flexors) to relieve contributing tension.
-
Consider incorporating nerve-gliding (“flossing”) techniques once irritation subsides, to restore healthy mobility of the ulnar nerve (within professional scope and tolerance).
-
Reinforce ergonomic education such as avoiding prolonged elbow flexion, pressure on elbows, or sleeping with arms bent tightly.
-
-
Complementary manual approaches:
-
Address muscle imbalance around the cervical spine and shoulder girdle.
-
Encourage thoracic mobility and scapular stabilization to optimize neural pathway spacing.
-
Safety & Referral
-
Refer for further assessment if:
-
There are progressive sensory/motor deficits in the hand or arm.
-
Symptoms worsen with conservative care or extend proximally into the neck/chest.
-
There are red flags for systemic or central nervous system involvement.
-
-
Avoid testing or manual therapy during acute inflammation or trauma to the nerve.