Anterior Drawer Test (Ankle)
The Anterior Drawer Test of the ankle is an orthopedic examination used to assess stability of the lateral ankle joint—specifically, the integrity of the anterior talofibular ligament (ATFL). This ligament is most commonly injured in lateral ankle sprains. The test helps identify both acute rupture and chronic laxity of the ATFL.
How the Test is Performed
-
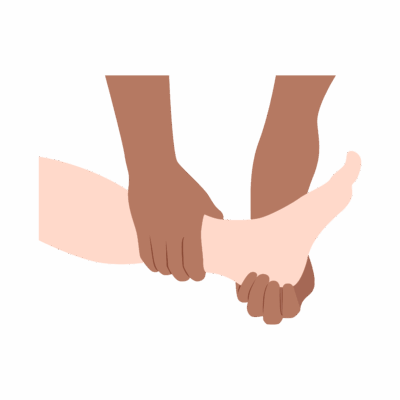
Client position: Supine or seated, with the knee slightly flexed (to relax the calf muscles), and the ankle positioned in ~10–20° of plantarflexion.
-
The examiner stabilizes the distal tibia/fibula with one hand, then uses the other hand to grasp the calcaneus/heel and attempts to draw the foot forward (anteriorly) relative to the tibia.
-
The examiner assesses:
-
The amount of anterior translation (shift) compared to the uninjured side
-
The quality of the end-feel, noting if it is firm (normal/ligament intact) or soft (ligament compromised).
-
-
Positive test: Increased anterior translation (often >1 cm) and/or a soft or absent end-feel compared to the contralateral side, indicating partial or complete ATFL tear.
-
Some variants use a prone position or a “clunk” sensation may be noted as the talus subluxates and relocates in the ankle mortise.
Clinical Significance
-
A positive test suggests ATFL sprain/rupture, mechanical ankle instability, or hypermobility—most common after inversion injuries.
-
The test is most sensitive and specific in acute injury settings (within days of injury), but may be less reliable for chronic laxity.
-
Diagnostic accuracy improves when combined with palpation and other physical exams (Talar Tilt Test, palpation for ATFL tenderness, presence of swelling).
Assessment
-
Use this test for clients with acute or chronic lateral ankle pain, instability, history of rolling the ankle, or recurrent sprains.
-
Document:
-
Side-to-side differences
-
Degree of translation and end-feel
-
Presence or absence of pain, swelling, or “clunk”
-
Functional limitations during gait or weight-bearing
-
Treatment
-
If positive:
-
Avoid vigorous manual therapy, aggressive mobilization, or strong stretching/massage near the lateral ligaments in acute or unstable ankles.
-
Use gentle soft tissue work, edema management, pain control, and gradual progression to functional strengthening and proprioceptive retraining.
-
Educate clients about ankle bracing, taping, activity modification, and proprioceptive exercises to prevent recurrent sprain.
-
-
Collaborate with physiotherapists for structured rehabilitation, balance training, and return-to-sport guidance if needed.
Safety and Referral
-
Refer for medical or orthopedic assessment if acute, severe instability, persistent pain, or recurrent sprains are present, or for imaging to rule out fractures or syndesmotic injury.
-
Monitor for signs of chronic instability and educate clients about long-term prevention strategies.