Apley’s Distraction Test
The Apley’s Distraction Test is a prone knee test used to assess ligamentous structures of the knee (collateral and cruciate ligaments), and is commonly paired with Apley’s Compression (Grind) Test, which biases the menisci.
How the Test is Performed
Clinically (orthopedic/physio context):
-
Position:
-
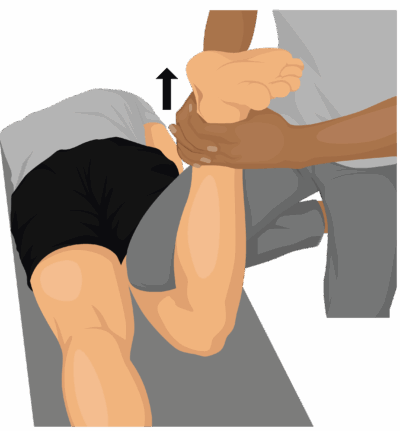
Client lies prone.
-
Knee of the test leg is flexed to about 90°.
-
-
Stabilization:
-
Examiner stabilizes the posterior thigh (often using their own knee or hand to fix the femur against the table).
-
-
Distraction + Rotation:
-
Examiner grasps the distal leg/ankle, applies axial traction (pulling upward) through the tibia, and simultaneously internally and externally rotates the tibia.
-
Therapist notes pain, excessive rotation, or sense of separation in the joint.
-
-
Comparison:
-
Repeat on the contralateral limb for baseline.
-
Clinical Significance
-
Positive Apley’s Distraction Test:
-
Pain or increased movement with distraction and rotation suggests injury or laxity of:
-
Collateral ligaments (MCL/LCL)
-
Possibly capsule / cruciate ligaments if deep joint pain is provoked.
-
-
-
Differentiation from meniscal pathology:
-
If compression (grind) is painful but distraction relieves or does not provoke pain, meniscal injury is more likely.
-
If distraction reproduces pain, ligamentous involvement is implicated.
-
Assessment
A massage therapist generally will:
-
Use this test as a screening adjunct, not as a stand‑alone diagnostic:
-
Indications: history of knee trauma, complaints of joint line pain, sensations of instability, or localized ligament tenderness.
-
-
Observe and note:
-
Location and quality of pain (medial, lateral, deep joint).
-
Sense of excessive laxity/“gapping” versus a firm end‑feel.
-
Comparison to the non‑symptomatic side.
-
-
Integrate with:
-
Other orthopedic screens (valgus/varus stress, McMurray/Thessaly, palpation, ROM) before forming working hypotheses and deciding if referral is needed.
-
Treatment
If Apley’s Distraction suggests ligament involvement:
-
Acute or unstable stage:
-
Avoid:
-
Deep friction directly over injured ligament.
-
High‑load stretching or aggressive ROM into end‑range rotation or varus/valgus.
-
-
Do:
-
Gentle soft tissue work to surrounding muscles (quads, hamstrings, gastroc, IT band) to reduce guarding.
-
Support edema management (if appropriate and not in conflict with acute injury protocols).
-
Respect bracing/taping and any weight‑bearing restrictions.
-
-
-
Subacute/chronic stage (medically cleared):
-
Use:
-
Progressive, symptom‑guided soft tissue techniques to address compensatory tension.
-
Work that supports alignment and neuromuscular control (e.g., hip and ankle musculature that influence knee mechanics).
-
-
Collaborate with physio for strength/proprioception (e.g., collateral and dynamic stabilizers).
-
Safety and Referral
-
Do not perform Apley’s Distraction Test if:
-
Known or suspected fracture, recent surgery, acute infection, or significant effusion.
-
Marked instability or locking that has not been evaluated medically.
-
-
Red flags / reasons to refer:
-
Audible pop at injury onset with immediate swelling and inability to bear weight.
-
Gross laxity or giving‑way with light manual stress.
-
Persistent locking, catching, or true joint blocking.
-
Night pain, systemic symptoms, or suspected inflammatory arthropathy.
-
-
In all such cases, defer intensive knee work and refer to a physician or physiotherapist for imaging and formal diagnosis before continuing localized treatment.