Bragard’s Test
Bragard’s Test is an orthopedic maneuver designed to confirm nerve root irritation, particularly of the sciatic nerve due to lumbar disc herniation or radiculopathy. It is considered a refinement or adjunct to the classic Straight Leg Raise (SLR) Test.
How the Test is Performed
-
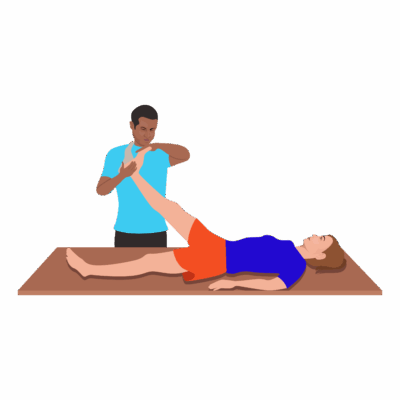
Client position: Supine (lying on the back), both legs straight.
-
The therapist performs a Straight Leg Raise on the affected side, noting the angle where radiating pain or symptoms occur (typically between 30°–70° of hip flexion).
-
The leg is then lowered slightly (about 5–10 degrees) from the symptomatic angle, until discomfort resolves.
-
The therapist then passively dorsiflexes the foot (bringing toes toward the head) while holding the hip and knee in position.
-
A positive Bragard’s Test: Reproduction of radiating pain, burning, tingling, or numbness in the same distribution as the original SLR.
-
If only calf tension (not radiating pain) is produced, it is considered negative for nerve involvement and more suggestive of hamstring or muscular tightness.
Clinical Significance
-
A positive test points to nerve root compression (L4–S1), sciatic nerve irritation, or lumbar disc herniation.
-
Helps differentiate neural tension from muscle or joint causes of posterior leg pain, such as tight hamstrings or hip pathology.
-
Sensitivity and specificity are moderate (sensitivity ~22–92%, specificity ~43–100% depending on studies and populations).
-
Also used as a tool to assess non-organic pain or to distinguish malingering (symptoms usually absent in non-organic causes).
Assessment
-
Use Bragard’s Test when a client presents with low back pain, radiating buttock/leg symptoms, suspected sciatica, or following a positive SLR.
-
Document the precise angle, symptom description, and whether the test reproduces classic neural pain or only stretches the calf.
Treatment
-
If positive (radiating neural pain):
-
Avoid vigorous or deep techniques to the lumbar spine, piriformis, or sciatic pathway that could exacerbate irritation.
-
Focus on gentle modalities, pain-modifying techniques, and education regarding posture and activity modification.
-
Collaborate with physiotherapists and refer for further assessment/imaging if symptoms are marked or progressive.
-
-
If negative: May indicate muscular tightness or non-nerve cause. The therapist should perform gentle stretching and myofascial release as tolerated.
Safety and Referral
-
Refer promptly if there is significant, progressive, or functionally limiting neural pain, persistent weakness, or “red flag” symptoms (saddle anesthesia, bowel/bladder incontinence, severe motor loss).
-
Provide clear documentation for interdisciplinary care and outcome monitoring.