Ely’s Test
Ely’s Test is an orthopedic muscle length assessment primarily used to evaluate the flexibility or contracture of the rectus femoris muscle (one of the quadriceps muscles) in the anterior thigh. It is commonly used to help diagnose muscle tightness related to stiff knee gait, postural changes, or anterior pelvic tilt, especially relevant in athletes, people with low back pain, or neurological conditions such as cerebral palsy.
How the Test is Performed
-
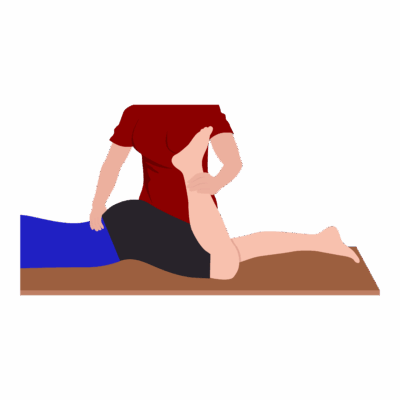
Client position: Prone (lying face down) on the exam table.
-
The examiner passively flexes the knee on the tested side, bringing the heel toward the buttock while stabilizing the pelvis.
-
The key observation is whether involuntary hip flexion occurs (the pelvis rises off the table as the knee bends), indicating rectus femoris tightness or contracture.
-
A negative test shows little or no pelvic movement and the heel can reach the buttock without compensation.
Clinical Significance
-
Positive Ely’s Test: Involuntary hip flexion or anterior pelvic tilting during passive knee flexion. This would be indicative of rectus femoris (and potentially quadriceps) tightness or contracture.
-
Helps distinguish rectus femoris tightness from iliopsoas (hip flexor) tightness, which is tested with the Thomas Test.
-
Relevant for assessing muscle length in individuals with low back pain, pelvic postural dysfunction, hip/knee pain, or neurological spasticity (e.g. cerebral palsy).
Assessment
-
Use Ely’s Test for clients with anterior pelvic tilt, stiff knee gait, anterior thigh/knee pain, or limited knee flexion during walking.
-
Document the degree of hip movement, any asymmetry, and pain or resistance for tracking outcomes.
Treatment
-
If positive:
-
Avoid aggressive stretching or deep soft tissue work on a highly contractured or actively painful rectus femoris.
-
Focus on gentle soft tissue release, slow graded stretching, and myofascial release for the quadriceps group, incorporating gluteal and hip stabilization work as needed.
-
Educate on home stretching, activity modification, and gradual postural correction, especially for chronic or neurological cases.
-
-
Instruct clients on exercises that restore rectus femoris length and support pain-free knee flexion and hip extension.
Safety and Referral
-
Refer for further evaluation if contracture is severe, bilateral, or not responsive to conservative therapy. This is especially in neurological or pediatric populations.
-
Collaborate with physiotherapists, sports physicians, or rehab professionals for persistent or complex cases.