Roos Test
The Roos Test—also known as the Elevated Arm Stress Test (EAST)—is a clinical provocation test used to help identify thoracic outlet syndrome (TOS), which involves compression of the neurovascular bundle as it passes through the thoracic outlet. It is considered one of the most sensitive tests for neurogenic TOS and evaluates all three intervals where the brachial plexus travels.
 How the Test is Performed
How the Test is Performed
-
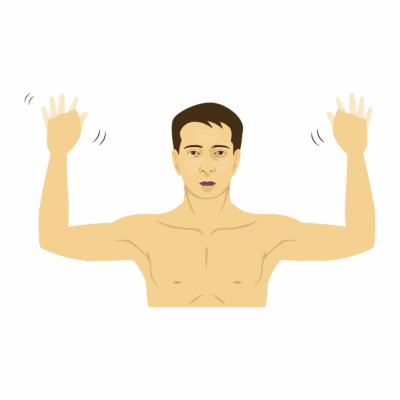
Client position: Sitting or standing, both arms elevated to 90° abduction and external rotation, elbows bent to 90°, so the arms are in the “goalpost” or “stick-up” position.
-
Execution:
-
The client is asked to open and close their hands repeatedly (at a moderate speed) for up to 3 minutes.
-
The test is monitored for emerging symptoms and the ability to complete the duration.
-
-
Positive test:
-
Reproduction of the client’s typical symptoms (pain, numbness, tingling, weakness, heaviness, ischemic pain, or discoloration) in the arm/hand within the test period, or the inability to sustain the position due to distress.
-
-
Minor forearm fatigue is not considered a positive test; true positives involve symptoms throughout the entire upper extremity or a return of the client’s familiar neurovascular complaints.
Clinical Significance
-
The Roos Test is designed to provoke symptoms by narrowing the scalene triangle and increasing vascular/neural compression.
-
Sensitivity is high (~84%), meaning it reliably detects TOS when present, but specificity is lower (~30%), meaning false positives can occur.
-
Positive Roos test findings may reflect neurogenic TOS (most common—brachial plexus compression), arterial TOS (pallor, ischemic pain), or venous TOS (cyanosis, swelling).
-
It helps with differential diagnosis:
-
Carpal tunnel syndrome may cause numbness only in the first three fingers.
-
Orthopedic shoulder issues may result in localized pain, but not forearm/hand symptoms.
-
Assessment
-
Use this test for clients with:
-
Numbness, tingling, pain, weakness, or swelling in the arm/hand—especially those worsened by overhead activities or posture.
-
Suspected TOS, postural dysfunction, or repetitive overhead work/lifting.
-
-
Document onset, duration, and distribution of symptoms, and ability/inability to complete the 3-minute protocol.
Treatment
-
If positive:
-
Avoid deep compressive work over the scalene triangle, first rib, clavicle, or pectoralis minor in acute/symptomatic clients.
-
Focus on gentle myofascial release, posture correction, and soft tissue decompression in the anterior neck, chest wall, and upper shoulder.
-
Educate about posture, ergonomics, and activity modification to reduce provocation of symptoms.
-
Gradual stretching, neural gliding, and thoracic spine mobility can be introduced with caution and as tolerated.
-
Safety and Referral
-
Refer to a physician, physiotherapist, or vascular specialist if the client has:
-
Severe, progressive, or disabling neurovascular symptoms,
-
Loss of color or circulation,
-
Inability to complete the Roos Test due to distress,
-
Associated swelling or prominent vascular changes.
-
-
Use in combination with other TOS tests—Adson’s, Wright’s, costoclavicular—to increase diagnostic accuracy.