Shoulder Depression Test
The Shoulder Depression Test is a clinical orthopedic test primarily used to assess for nerve root irritation, compression, or brachial plexus injury (often cervical radiculopathy). It reproduces symptoms by stretching the nerve roots and soft tissues on the side of the neck, offering insight into possible underlying nerve compromise.
How the Test is Performed
-
Client position: Seated (most common), but can also be performed standing or supine.
-
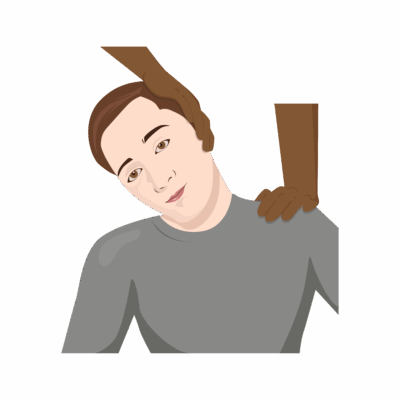
The examiner gently side flexes the client’s head to one side (away from the side being tested).
-
The examiner then applies downward (depressive) pressure on the opposite shoulder (the side being tested), creating a stretch of the cervical nerve roots and brachial plexus.
-
The client is asked to report any symptoms (radiating pain, numbness, tingling) in the stretched arm or along the neck.
-
A positive test: Reproduction of the client’s usual arm or neck pain, or new radicular symptoms (radiating into the arm/hand).
Clinical Significance
-
A positive Shoulder Depression Test suggests nerve root compression/irritation, possible foraminal encroachment, adhesions of dural sleeves, or brachial plexus traction injury.
-
It can help differentiate radicular (nerve root) pain from local muscular or capsular restriction.
-
The test can also support diagnosis of cervical facet irritation and differentiate plexopathies from true radiculopathies, depending on symptom distribution.
Assessment
-
Use this test for clients with:
-
Neck pain, arm pain, or symptoms radiating from the neck to the hand
-
Suspected nerve involvement (numbness, tingling, or weakness in the arm)
-
History of traumatic neck injury or postural complaints
-
-
Document which side is tested, the presence and distribution of symptoms provoked, and their comparison to the client’s original complaints.
Treatment
-
If positive:
-
Avoid deep, forceful, or compressive manual therapy to the cervical region or shoulder girdle when nerve compromise is suspected.
-
Focus on gentle soft tissue work, pain modulation, and reduce tension in superficial cervical and shoulder muscles.
-
Educate about posture, cervical spine ergonomics, and home-care strategies to minimize nerve root provocation.
-
Refer for medical/physiotherapy assessment if progressive neurological findings, persistent severe pain, or new motor/sensory deficits develop.
-
Safety and Referral
-
Immediate referral is required if there is evidence of progressive weakness, sensory loss, loss of reflexes, or signs of spinal cord involvement (such as loss of bowel/bladder control).
-
Collaborate with healthcare team for interdisciplinary management if radiculopathy, plexopathy, or significant nerve involvement is confirmed