Thomas Test
The Thomas Test is a classic orthopedic assessment used to evaluate hip flexor muscle length and flexibility, primarily the iliopsoas and rectus femoris, as well as to identify hip flexion contracture, anterior pelvic tilt, or lower back/postural dysfunction. It is often used in clients with lower back pain, hip pain, or postural/movement restriction.
How is the Test Performed
-
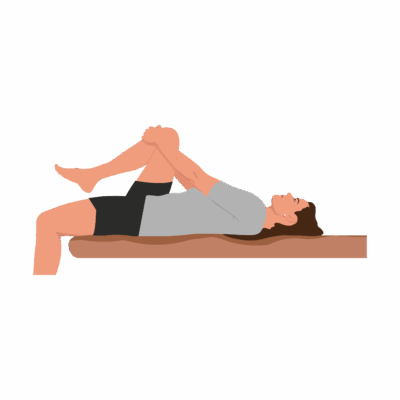
Client position: Supine (lying on their back) near the edge of the treatment table.
-
The client flexes one hip (brings knee toward the chest) and holds it with both hands, flattening the lumbar spine and pelvis against the table.
-
The other leg is allowed to relax and extend fully, hanging off the edge of the table.
-
Key observations:
-
If the thigh of the extended leg does not touch the table, there is iliopsoas tightness or a hip flexion contracture.
-
If the knee extends (>90° flexion) instead of resting in natural flexion, rectus femoris tightness is likely.
-
If the leg abducts or externally rotates, this may indicate tightness of the tensor fasciae latae or iliotibial band.
-
Lateral rotation of the tibia during the test may indicate biceps femoris tightness.
-
Clinical Significance
-
A positive test (inability of the extended thigh to lay flat on the table, or knee extension/lateral deviation) indicates loss of hip muscle flexibility due to iliopsoas, rectus femoris, TFL, or ITB tightness.
-
It helps differentiate the specific muscle group involved in restricted hip extension.
-
Identifying these restrictions is essential for targeted mobility, stretching, and posture programs, and may help address postural dysfunction, gait abnormalities, anterior pelvic tilt, or persistent back pain.
Assessment
-
Use the Thomas Test for clients with anterior pelvic tilt, low back pain, hip/postural restrictions, or movement dysfunction.
-
Perform bilateral testing for side-to-side comparison and thorough assessment.
Treatment
-
If positive for tightness:
-
Do not overstretch or use aggressive techniques on identified tight/contractured muscles, especially if acute pain is present.
-
Focus on gentle soft tissue release, myofascial work, graded stretching, and active mobility exercises for involved hip flexors, quadriceps, TFL/ITB as needed.
-
Educate clients about home stretching, posture awareness, and activity modifications to avoid aggravating hip flexor tightness.
-
Integrate pelvic stabilization, gluteal activation, and lumbar support in ongoing care plans for postural dysfunction.
-
-
Re-assess after treatment to track progress and direct further intervention.
Safety and Referral
-
Refer for medical/physiotherapy evaluation if contracture is severe, bilateral, painful, or not responsive to conservative management.
-
Work collaboratively with rehab professionals for complex or post-surgical hip/lumbar conditions