Vocal Fremitus Test
The Vocal Fremitus Test (often called tactile vocal fremitus) is a respiratory assessment used to feel how well vibrations from a client’s voice are transmitted through the lungs and chest wall.
Changes in vibration intensity can indicate altered lung tissue density (e.g., consolidation) or air/fluid in the pleural space.
How the Test is Performed
In a medical/respiratory exam (not typically within massage scope):
-
The client sits or stands upright.
-
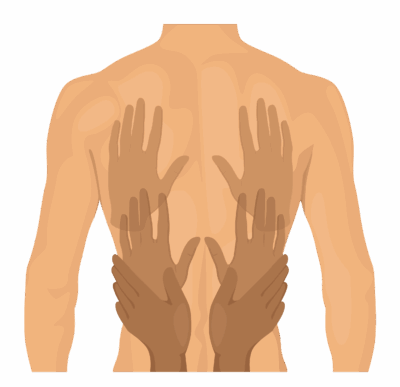
The examiner places the ulnar border or palm base of both hands symmetrically on the chest or back.
-
The client repeatedly says a low‑frequency phrase (commonly “ninety‑nine” or “one, two, three”) in a steady tone.
-
The examiner palpates over multiple lung regions, comparing side‑to‑side for vibration intensity from apices to bases, anterior and posterior.
-
Findings:
-
Increased fremitus = stronger vibrations than normal.
-
Decreased/absent fremitus = weaker or missing vibrations.
-
Massage therapists generally do not perform this test formally, but can understand the concept.
Clinical Significance
-
Increased vocal/tactile fremitus
-
Suggests increased lung tissue density, often due to consolidation (e.g., lobar pneumonia, some tumors, lobar collapse).
-
-
Decreased or absent fremitus
-
Suggests air or fluid around the lung (e.g., pneumothorax, pleural effusion) or very hyperinflated lung (e.g., advanced COPD, asthma).
-
These are medical respiratory conditions, not musculoskeletal problems, and require medical evaluation.
Assessment
For massage therapists, vocal fremitus is contextual information, not a primary assessment tool:
-
Listen to the client’s history:
-
Chronic cough, recurrent bronchitis/pneumonia, COPD, asthma, unexplained shortness of breath, or chest pain with breathing.
-
-
Informally, you may notice chest vibrations (e.g., when your hands are on the thorax and the client talks or laughs), but this is incidental—not a diagnostic maneuver.
-
If the client reports recent imaging or tests (e.g., pneumonia, pleural effusion, lung collapse), you can factor that into treatment planning and positioning, but diagnosis remains strictly medical.
Treatment
When lung pathology is known/suspected:
-
Modify or limit thoracic work:
-
Use gentle pressure over ribs and sternum; avoid deep, sustained compression over acutely painful or compromised areas.
-
-
Focus on:
-
Breathing‑supportive techniques (gentle rib cage mobilization, soft tissue work to accessory breathing muscles: scalenes, intercostals, pectorals, diaphragm region) when medically cleared.
-
Postural work (thoracic extension, scapular mobility) that may ease breathing mechanics.
-
-
Avoid:
-
Aggressive percussive techniques over lungs in clients with fragile respiratory status unless explicitly recommended by their healthcare team.
-
Massage can complement medical care by reducing accessory muscle overuse, anxiety, and general tension, which often improves perceived breath ease.
Safety and Contraindications
For massage therapists, key safety points:
-
Absolute red flags requiring medical referral/deferral of massage:
-
Acute, unexplained shortness of breath at rest or with minimal exertion.
-
New onset or rapidly worsening chest pain, especially with breathing.
-
Signs of respiratory distress (labored breathing, cyanosis, inability to speak in full sentences).
-
-
Relative cautions:
-
Recent pneumonia, pleural effusion, pneumothorax, pulmonary embolism, or major thoracic surgery—work only after medical clearance, gently, and away from acute sites.
-
-
Do not attempt to “re‑test” or interpret fremitus differences yourself as a diagnostic judgment.
-
Document any concerning respiratory symptoms reported during intake and recommend the client follow up with their primary or emergency care provider when indicated.